Study Shows How Doctors GET PAID to Fuel the Opioid Crisis

Most doctors are wonderful people and consummate professionals who truly want the best for their patients. But a recent study suggests much of the blame for the opioid crisis lies squarely on the shoulders of doctors who write prescriptions for hard-hitting opioids when other simpler pain-relieving methods would suffice.
The study shows that as recently as 2015, doctors were still prescribing the addictive and potentially deadly painkillers even for minor injuries in great numbers.
Researchers wrote in the Annals of Emergency Medicine that 1/4 of patients treated for ankle sprains between 2011 and 2015 were prescribed an opioid to deal with the pain.
For the study, researchers from the University of Pennsylvania analyzed private insurance claims filed by nearly 31,000 patients who had been treated in the emergency room for a sprained ankle. The patients were over the age of 18 and had not been prescribed an opioid in the 6 months prior to their injury.
Researchers looked at prescriber habits shortly before 2016, when the U.S. Centers for Disease Control and Prevention (CDC) issued guidelines urging doctors to only prescribe opioids in dire situations and the federal government announced it would limit the length of first-time opioid prescriptions. [2]
Read: The DEA Will Slash Opioid Production 25% in 2017
Study leader Kit Delgado, an assistant professor of emergency medicine and epidemiology at the University of Pennsylvania’s Perelman School of Medicine, said:
“There was this leap to opioids, either in perception of patient expectations or to meet patient expectations.”
The team found that:
- Overall, 25.1% of the patients studied received an opioid prescription.
- Most of the opioid prescriptions were for short-term use – about 15 pills (enough for 3 days) and low-dose. However, a small number of patients received a prescription equivalent to more than 30 tablets of medium-strength oxycodone – a drug with “high potential for abuse,” according to the Drug Enforcement Agency (DEA).
- Nearly 5% of patients who received a mid-strength opioid prescription progressed to prolonged opioid use, compared to about 1% of patients who were given a more moderate prescription, and 0.5% of patients who did not receive an opioid prescription.
Where a patient lived played a significant role in whether or not they would be prescribed one of the powerful analgesics. In Arkansas, 40% of patients left the ER with an opioid prescription, compared to just 3% of patients in North Dakota. All but 1 of the 9 states that recorded above-average opioid prescribing is in the South or Southwest. [1] [2]
Above-average prescribing was documented in North Carolina, Tennessee, Georgia, Alabama, Arkansas, Texas, Oklahoma, Kansas, and Arizona. [2]
Fortunately, during the study period, overall prescription rates fell from 28% of patients in 2011 to 20.4% in 2015. [1]
Read: Opioid Prescriptions Down for 1st Time in 20 Years
Most opioid prescriptions are written by primary care physicians; emergency room doctors are a blip on the entire map. Overall, there were about 215 million prescriptions for the painkillers in 2016, according to the CDC. [2]
In light of the opioid epidemic that wipes out thousands of lives a year in the U.S., why did doctors prescribe such addictive drugs in such large amounts and doses to so many people? There are 4 possible explanations.
Read: This NJ Hospital Will Do Anything to Avoid Prescribing Opioids
Freebies and Financial Perks
No one likes to think their doctor is prescribing them a drug because he or she stands to gain from it, but the disturbing reality is that it happens all the time.
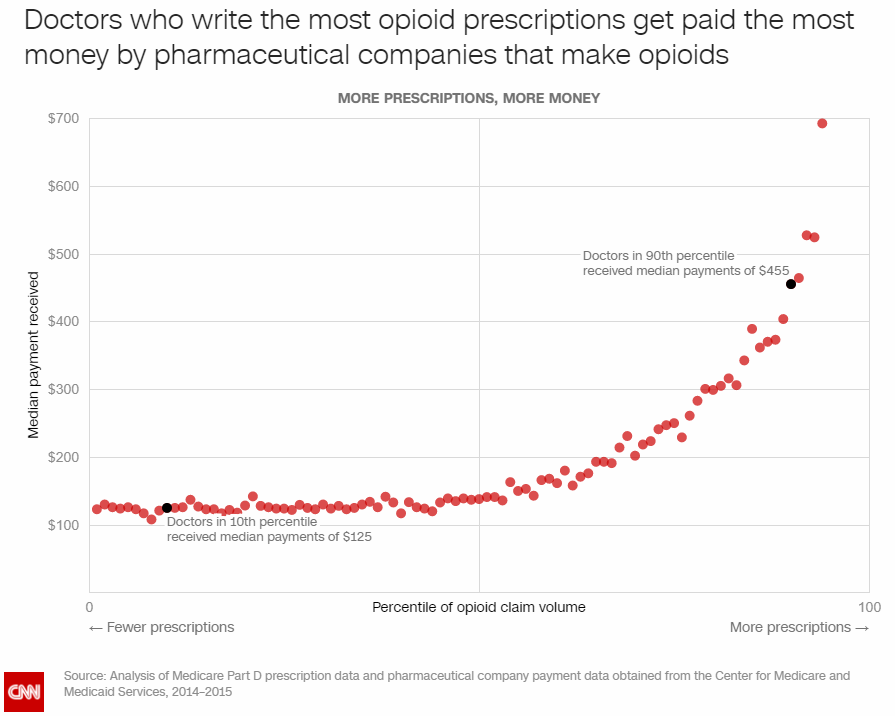
In 2014 and 2015, opioid makers had no problem paying doctors 6-figure sums for speaking, consulting, and other services. The companies paid thousands of other dollars $25,000 sums during that time. [3]
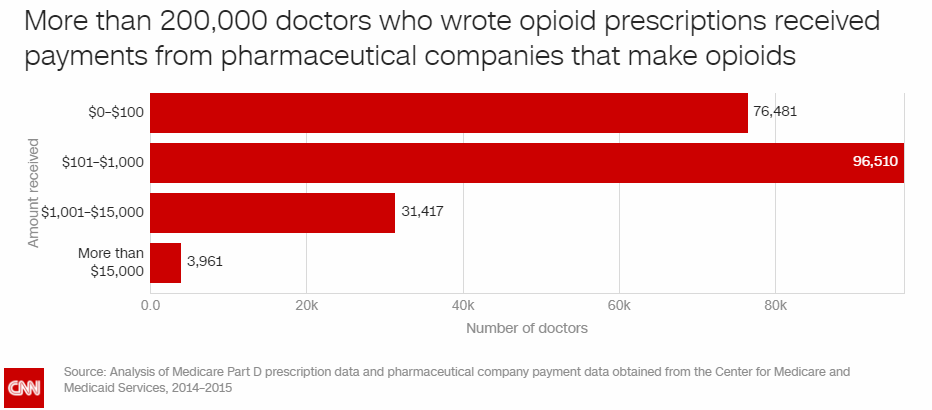
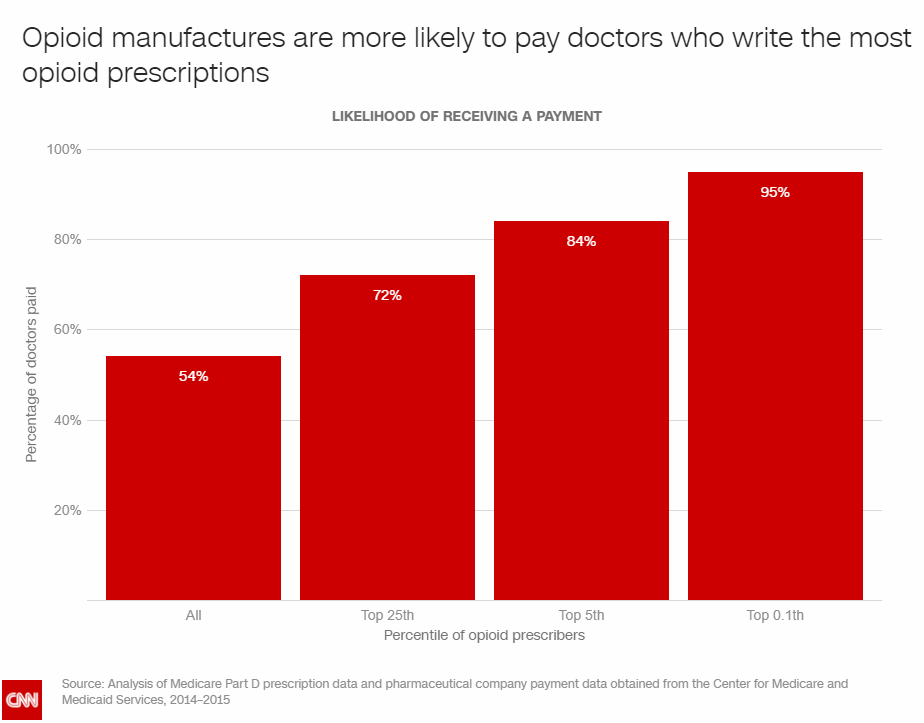
Doctors who hocked the most pain pills to their patients were the most likely to bring in big bucks. It’s not hard to imagine how tempting a 6-figure sum could be to someone with a prescription pad. It’s also not hard to imagine how a doctor would feel beholden to a pharmaceutical company after being paid such exorbitant amounts.
You could almost say the drug companies were the drug kingpins, the doctors were the dealers, and in tragically too many cases, the patients became – unwittingly – the junkies. And if the dealers wanted to get paid, they had to keep moving the kingpins’ product.
Ignorance
It’s possible that some of those doctors during the study period offered more opioids because they lacked the medical training to know the full addictive nature of the drugs. [2]
It is a doctor’s job to ease suffering, after all, and physicians have been taught to aggressively treat pain.
In 1980, a 101-word letter written by Boston University Medical Center researchers published in the New England Journal of Medicine, served as the foundation for doctors’ opioid prescribing habits for decades.
In the letter, the scientists claimed that “despite widespread use of narcotic drugs in hospitals, the development of addiction is rare in medical patients with no history of addiction.”
Based on these promises of safety, opioid prescriptions exploded.
The scientists went on to say in the letter that in a review of 11,882 hospitalized patients treated with narcotics, they found “only four cases of reasonably well-documented addiction.”
That letter went on to be cited in hundreds of reputable medical journals.
Clueless Prescribing
Doctors don’t always know how many pills to prescribe in individual cases. [2]
A Yale University study found that hospitals were able to successfully decrease opioid prescriptions by going into electronic medical records and lowering default settings for pill limits.
Previous studies show that when surgeons have specific guidelines for how many pills they should prescribe after common procedures, opioid use decreased sharply.
Yet other studies show that long-time use may partly depend on whether an individual was treated by a “low-intensity” or a “high-intensity” prescriber in the ER.
Ego
Anyone can go online and give a doctor a positive or negative review. Delgado and his colleagues believe that in some cases, doctors prescribe more opioids in pursuit of glowing reviews.
Sources:
[1] Time
[3] CNN
Well that is just fine and dandy. How about people like me who should definitely not take NSAID due to heart attack risk? I am finishing up breast cancer treatments and had to BEG my oncologist for 5, 5mg Oxycodone to replace ones that I had to take for my breast abscess due to the radiation treatment I had following a lumpectomy. I have chronic pain. I do not want to take Lyrica due to the side effects and long term health effects. I’m 64 years old and am SO tired of the pain! Both knees are replaced, I have reduced 4 bulging discs to only one through my own PT of kayaking, have a frozen shoulder, cannot take Vicodin. Everything I can do, I have done to reduce my pain. Now, in addition to the cancer, I have psoriatic arthritis attacking my joints. I can’t believe what a person has to go through due to the current opioid climate! I have terrible rebound headaches from Feverfew. So, I guess it will be a wheelchair for me before long…. I wonder how many of the opioid deaths have actually been suicides??? It’s hell to be in pain and have the doctors say they can’t give pain meds due to the risk of being investigated….